Kudos to the Center for Effective Philanthropy for its recent report, Policy Influence: What Foundations Are Doing and Why, which documents the growing commitment to policy engagement in the philanthropic sector. As the nation navigates the COVID-19 pandemic, an economic collapse, and mass protests against racism and police violence, philanthropic efforts to influence decision-making on policy are needed now more than ever.
The results of CEP’s important research are highly consistent with our analytic efforts at Grantmakers In Health (GIH), where I serve as a program advisor. Over the last two decades, GIH has observed a significant increase in the number of health foundations seeking to inform and influence public policy decisions, as well as the range of strategies funders are adopting to accomplish this goal.
GIH Funding Partners are diverse, with assets ranging from under $1 million to over $11 billion and annual health-related giving ranging from $100,000 to $400 million. Roughly 50 percent of GIH Funding Partners fund at the local level (e.g., neighborhood, city, county, or multi-county area), 30 percent fund at the state level, and 20 percent fund at the national level. All GIH Funding Partners have identified the promotion of health and wellbeing as central to their missions, but priorities vary widely, with focus areas including expanding access to healthcare services, advancing health equity, improving the quality and efficiency of care, promoting healthy eating and active living, targeting under-resourced aspects of health (such as behavioral health and oral health), and addressing the needs of vulnerable populations (such as children and older adults).
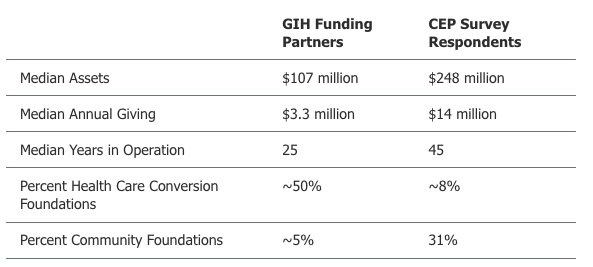
The makeup of GIH’s Funding Partner network differs from the demographic profile of foundations that responded to CEP’s survey. Relative to the CEP sample, GIH Funding Partners tend to have smaller asset sizes, lower annual giving levels, and are typically “younger” organizations that have been in operation for fewer years (see Figure 1). Not surprisingly, a much larger portion of GIH Funding Partners are healthcare conversion foundations (about 50 percent) compared to the 8 percent of respondents included in the CEP sample.
FIGURE 1: Demographics of GIH Funding Partners v. CEP Survey Respondents
Despite these fairly substantial differences, health funders in the GIH network exhibit many of the same perspectives, concerns, and challenges highlighted in CEP’s study. While the report was broadly relevant to the experience of health philanthropy, a few of CEP’s findings resonated with me in particular.
Policy engagement is widely prevalent among philanthropic organizations. CEP found that 90 percent of philanthropic leaders report that their foundations seek to influence public policy. CEP acknowledged that this high level of policy engagement is likely driven in part by response bias, but GIH has observed similar levels of policy engagement among health funders, suggesting CEP’s estimates are not far off the mark.
For example, a study conducted by GIH in 2015 found that 70 percent of local health funders supported or directly engaged in activities intended to inform or influence public policy, and an additional 10 percent planned to become policy engaged in the near future. (This analysis was based on a random sample of local funders with a 100 percent response rate, although the sample size was not large enough to be statistically representative.)
My sense is that the vast majority of GIH Funding Partners would describe their organizations as policy engaged, although the nature and magnitude of that engagement varies considerably. This dynamic represents a real sea change in the field; twenty years ago, relatively few health funders viewed policy change as an important element of their mission.
A number of factors have contributed to health funders’ embrace of policy-change strategies. Influential developments include the passage and implementation of the Affordable Care Act in 2010; an expanding focus on improving the “upstream” determinants of health, such as housing, employment, and education; and the prioritization of health equity to address long-standing health disparities among communities of color and low-income populations. Health funders have recognized that advancing these ambitious goals requires a systems-change perspective, which necessitates policy engagement. Conversion foundations and other health funders with modest assets also understand that strategic investments in the policy arena can yield significant results at a feasible cost.
Policy-change strategies remain underutilized. While policy engagement is widespread, health funders do not always utilize the full array of policy change tools at their disposal.
Power-building strategies are particularly under-utilized. It was encouraging to see CEP report that 91 percent of responding foundations support community organization/grassroots mobilization and 64 percent support voter engagement. GIH’s 2015 study found that just 39 percent of local health funders support community organizing and very few respondents funded voter engagement activities. Anecdotal evidence suggests that state and national health funders may be more likely to support organizing and voter engagement than local health funders. However, it is doubtful that the field of health philanthropy collectively reaches the level of support for organizing and voter engagement reported by CEP.
Health funders do mirror CEP’s findings with respect to the limited use of general operating support for grantees’ policy efforts, as well as the widely prevalent use of unnecessary language in grant agreements that restrict the use of grant funds for lobbying efforts. In an unpublished survey of funders participating in GIH’s policy programming conducted in 2009, just 27 percent reported that they provide general operating support to policy advocacy organizations, and 64 percent reported organizational policies that restricted grantees’ ability to use funds for lobbying.
While more recent data for GIH Funding Partners are not available, I am not sure there has been much movement on either measure in the past decade. Advocacy organizations need to engage in lobbying in order to effect policy change, and foundations can do more to support these activities in legally permissible ways.
Barriers to more robust policy change efforts can be overcome. Like CEP respondents, GIH Funding Partners often cite board support as a major hurdle for policy engagement. Foundation trustees play a critical role in determining whether and how a funder will pursue policy change efforts. Years ago, I frequently heard concerns about both the evaluability of policy activities and legal restrictions on lobbying cited as reasons why foundation boards were not supportive of policy engagement. While these concerns still exist, they seem less common than they once were. Fears about appearing “partisan” now seem to be the major rationale for health foundation boards wary of exerting policy influence. Health policy has become highly politicized and foundation boards often see policy engagement as “taking sides” in these partisan debates.
Leaders of health foundations have been effective at building support for policy change within their governing boards through education, strategic visioning, and changes in board composition. A number of health foundation executives have taken deliberate steps to recruit board members who understand the power of policy engagement and will champion these approaches. Reconstituting board membership can sometimes be the only way to overcome entrenched opposition to policy-advocacy investments.
One final way in which GIH’s experience aligns with CEP’s is, unfortunately, in less than robust response rates to surveys of the field. At GIH, we have observed suboptimal responses to our survey efforts, despite attempts to simplify survey designs and facilitate response. It is not entirely clear why philanthropic organizations are reluctant to share their own practices and experiences. I suspect that this reticence reflects an overly cautious culture common among foundations. Funders are understandably protective of their reputational assets, but that protectiveness can too often lead to a lack of transparency.
I am hopeful that health philanthropy, along with the wider philanthropic sector in general, will continue to increase investments in policy-change strategies, and will further expand funding for more proactive forms of advocacy and power building. Additional analytic work, like CEP’s excellent contribution to the field, will be needed to monitor this evolution, document promising trends, and identify best practices. Too much is at stake for philanthropy to sit on the sidelines.
Eileen Salinsky is a program advisor at Grantmakers In Health (GIH).